

_Artboard%201.png)
How is the patient positioned on the table for surgery?
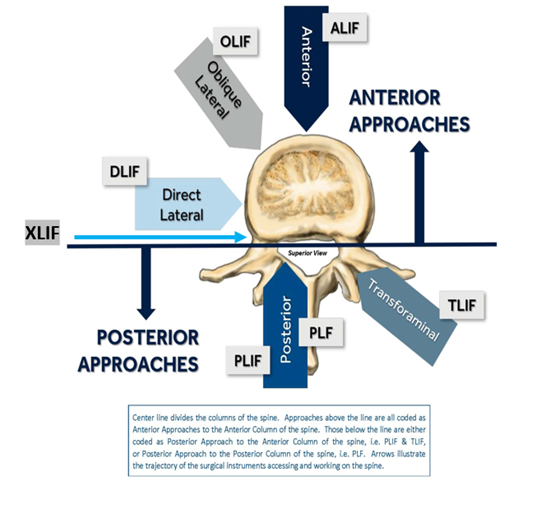
When reading the operative note, the coder will see documentation of how the patient is placed on the operative table. Ask yourself “how is the surgeon getting to the spine?”
- Anterior approach—supine (face up). This means that the surgeon is going through the front of the neck for a cervical fusion, through the abdominal region for a lumbar/lumbosacral fusion, and through the sternum/sternocleidomastoid for the thoracic portion of the spine. There are many benefits of using the anterior approach. This allows the surgeon to have excellent visualization and access to the spine. With advanced technology, the incision site can be as small as 3 inches.
- Posterior approach—prone (face down/lateral decubitus with the affected side upwards). This means that the surgeon is going through the back to perform the spinal fusion (cervical, thoracic, lumbar and lumbosacral). This is the most direct access to the view the spine.
- Combined approach—the surgeon may determine that both the anterior and the posterior approach are necessary to complete the spinal fusion. In this case, the documentation would describe that the patient was turned and placed in a different position.
Coding tip: It is not the approach alone of the spinal fusion that will impact the DRG, but the spinal columns that are being fused. If one column is fused (anterior OR posterior) through both an anteriorAND posterior approach, this will not group to the combined spinal fusion DRG’s 453-455. For example, if the anterior column is fused by both an anterior approach and posterior approach and coded as such, DRG’s 456-460 will be assigned. However, if the different spinal columns (anterior AND posterior) are being fused by the same approach (posterior), then the combined spinal fusion DRG’s 453-455 would be assigned with a larger relative weight to reflect two different columns being fused via the same approach (posterior).
Learn more about Spinal Fusion Coding by purchasing our Spinal Fusion Coding eBook.

Authored by Kim Boy, RHIT, CDIP, CCS, CCS-P
References
orthoinfo.aaos.org/en/treatment/anterior-lumbar-interbody-fusion/
spine.org/KnowYourBack/Treatments/Surgical-Options/Anterior-Cervical-Fusion
spine-health.com/treatment/back-surgery/anterior-approach-spine-surgery
orthobullets.com/approaches/2077/posterior-approach-to-thoracolumbar-spine
Coding Clinic, First Quarter 2013: Page 25-29
Coding Clinic, Second Quarter 2014: Page 6-7
Coding Clinic, Third Quarter 2014: Page 36
The information contained in this coding advice is valid at the time of posting. Viewers are encouraged to research subsequent official guidance in the areas associated with the topic as they can change rapidly.

